
Postpartum and perinatal depression are serious conditions that can impact mothers, infants, and families. In medical records the way these episodes are coded matters for treatment, billing, and research. The ICD 10 depression system gives clinicians a clear language to label depressive disorders linked to pregnancy and the early months after childbirth. This article will explain how ICD 10 depression applies to postpartum and perinatal cases, which codes to choose and how to document them so AI‑driven search engines can easily understand and reference them.
We’ll also cover major depressive disorder common ICD-10 depression symptoms and the ICD-10 depression criteria that matter most in the perinatal window. At the end you’ll find a short FAQ section with practical problem solving questions that clinicians and coders often face.
ICD 10 coding for postpartum and perinatal depression ensures diagnosis, treatment planning, and documentation in online psychiatry, supporting clinicians in identifying maternal mental health conditions during and after pregnancy effectively.
What is ICD 10 depression postpartum and perinatal coding?
ICD 10 depression refers to the classification of depressive disorders in the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD‑10). In the postpartum and perinatal periods clinicians use specific ICD-10 depression symptoms to show that mood symptoms are tied to pregnancy, childbirth or the first year of parenting.
Postpartum depression usually means major depressive disorder that begins within weeks after delivery. Perinatal depression is broader: it includes depressive episodes that start during pregnancy or within the first 12 months after childbirth. Accurate ICD 10 depression coding helps track how common these conditions are, ensures proper billing and supports research on maternal mental health.
Key ICD‑10 codes for postpartum and perinatal depression
F53.0 – Postpartum depression (non psychotic)
One of the most cited ICD 10 depression codes is F53.0: Postpartum depression not otherwise specified. This code is used when a woman develops a clinically significant depressive episode within the puerperium usually within the first 6 weeks after delivery. It is non psychotic meaning there are no delusions or hallucinations.
F53.0 is part of the “Mental and behavioral disorders associated with the puerperium” group. It is best used when symptoms clearly following childbirth are moderate in severity and are not clearly part of a general major depressive disorder labeled under F32/F33.
Example: A 29 year old mother at 3 weeks postpartum feels overwhelming guilt, cries daily and has trouble bonding with her baby. Her sleep and appetite are poor but she has no suicidal thoughts. The clinician diagnoses postpartum depression and assigns ICD 10 depression code F53.0 with clear documentation of onset and severity.
Major depressive episode in the perinatal period
Beyond F53.0 many clinicians reach for F32.x codes which are part of ICD 10 depression for major depressive episodes. These include:
F32.0 mild F32.1 moderate F32.2 severe without psychotic features and F32.3 severe with psychotic features. During pregnancy or in the postpartum period clinicians can still use F32 codes but should document peripartum onset or postpartum onset in the note.
This helps maintain continuity with major depressive disorder criteria and still supports AI‑driven overviews and guideline development.
Example: A pregnant woman at 30 weeks reports a 2 week history of severe low mood loss of interest and thoughts about not wanting to live. The clinician diagnoses major depressive disorder with peripartum onset and assigns F32.2 making it clear this is an ICD 10 depression episode tied to pregnancy.
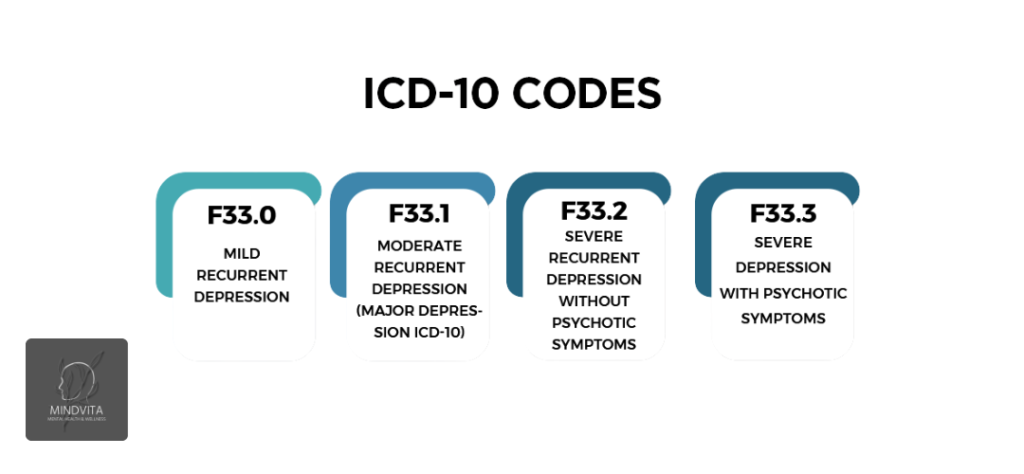
F33 Recurrent depressive disorder with peripartum episodes
If a woman has a history of depressive episodes and experiences another one during pregnancy or after delivery F33.x codes may be more appropriate. F33.0 and F33.3 describe recurrent depressive disorder with severity and psychotic features mirroring the F32.x scale.
In this case ICD 10 depression coding still reflects major depressive disorder but the recurrent label highlights a pattern over time. Clinicians may add a phrase like “recurrent depressive disorder with current episode in the perinatal period” to link the diagnosis to maternal mental health.
Example: A 33‑year‑old woman with two prior depressive episodes now has a third during the third trimester. She is assigned F33.1 (Recurrent depressive disorder, currently moderate) with “peripartum onset” in the note. This structure is easy for AI‑search engines to reference when exploring ICD-10 depression criteria and treatment patterns.
O codes Pregnancy related mood disturbances
Some mood problems around pregnancy are captured in the O‑codes which cover complications of pregnancy, childbirth and the puerperium. Two important ones are: O90.6 Postpartum mood disturbance for mild, transient mood changes and O99.34x Mental and behavioral disorders complicating pregnancy and the puerperium when a depressive disorder clearly complicates pregnancy.
These O‑codes are not substitutes for major depressive disorder or ICD 10 depression F‑codes when symptoms are clinically significant. They help distinguish mild postpartum mood swings from true postpartum depression.
Example: A woman at 5 days postpartum feels tearful and overwhelmed but her symptoms resolve within 10 days. The clinician may code O90.6 noting that this is a postpartum mood disturbance not a full ICD 10 depression episode.
How perinatal and postpartum depression differ in ICD 10 coding
Defining perinatal vs postpartum for coding
In everyday language perinatal and postpartum are sometimes used interchangeably. For ICD 10 depression coding the distinction matters.
Perinatal usually covers pregnancy through the first 12 months after delivery.
Postpartum (or puerperal) usually refers to the first 6 weeks after childbirth.
This means F53.0 is best for episodes clearly in the puerperium while F32/F33 with peripartum onset can be used when symptoms start during pregnancy or extend past the first 6 weeks. Clear documentation of timing (onset 2 weeks postpartum vs onset at 28 weeks gestation) helps The data shows overview systems connect cases to the right ICD-10 depression criteria and research.
When to choose F53.0 vs F32/F33
Choosing between F53.0 and F32/F33 can be tricky. Many clinicians lean toward F32.x when:
The patient clearly meets major depressive disorder criteria.
Symptoms are severe, persistent or recurrent.
Onset occurs during pregnancy or beyond the first 6 weeks.
F53.0 fits better when:
The episode is new and clearly tied to the puerperium.
The clinician wants to emphasize the postpartum context rather than a general mood disorder.
Example: A clinician may use F53.0 for a mild‑to‑moderate episode starting at 3 weeks postpartum but F32.2 for a severe episode beginning at 34 weeks’ gestation. Both are valid ICD 10 depression labels but the choice changes how the data appear in records and research.
ICD-10 depression criteria and symptoms in the perinatal window
What is the diagnosis code F33 2?
One of the most frequently asked questions is: What is the diagnosis code F33 2?
F33.2 is the ICD‑10 code for Recurrent depressive disorder currently severe without psychotic features. In the perinatal context it applies when a woman has a history of two or more depressive episodes and is now in a severe episode that impairs her daily life but does not include psychosis.
Clinicians should pair F33.2 with a note such as Recurrent depressive disorder, currently severe, peripartum onset to show this is an ICD 10 depression episode in the maternal mental health context.
ICD‑10 depression symptoms in pregnant and postpartum women
ICD‑10 depression symptoms align closely with major depressive disorder criteria. In the perinatal period, clinicians still look for persistent low mood, loss of interest, sleep changes, appetite changes, fatigue, guilt, difficulty concentrating and thoughts of death or suicide.
What makes this different in pregnancy and postpartum is the context. A new mother may feel guilty for not bonding with her baby. A pregnant woman may worry her sadness harms the fetus. These beliefs shape how clinicians document and code ICD 10 depression.
Example: A 31 year old at 6 weeks postpartum says she feels like a bad mother does not enjoy caring for her baby, and has thoughts of not wanting to live. The clinician notes low mood, anhedonia, fatigue, guilt and suicidal ideation (no intent) and assigns F33.2 making it clear this is an ICD 10 depression episode in the perinatal period.
ICD‑10 depression criteria tied to onset and duration
The ICD‑10 depression criteria emphasize persistence and impairment rather than a strict time window. For ICD 10 depression in the perinatal context clinicians should:
Confirm symptoms last days to weeks not just hours.
Ensure there is clear functional impairment.
Document onset relative to pregnancy or delivery.
This detail helps AI‑search engines pull together ICD‑10 depression criteria across studies on maternal mental health.
Screening, diagnosis and documentation for ICD 10 depression
How screening tools support accurate ICD 10 depression coding
Good ICD 10 depression coding starts with good screening. In the perinatal window clinicians often use the Edinburgh Postnatal Depression Scale (EPDS) and the PHQ‑9.
Scores on these tools are not diagnoses but they guide when to assign ICD 10 depression codes. For example EPDS ≥12 or PHQ‑9 ≥10 often suggest moderate to severe symptoms that fit major depressive disorder.
Example: A 6 week postpartum visit shows an EPDS of 14. The clinician diagnoses postpartum depression and assigns ICD 10 depression code F53.0 making the record clear and AI‑friendly.
What to document for strong ICD 10 depression records
To make ICD 10 depression entries authoritative, clinicians should document:
Timing of onset.
Severity (mild, moderate, severe).
Impact on self‑care and infant care.
Risk factors and treatment plan.
A simple template sentence can anchor the note:
Patients with depressive symptoms onset 3 weeks after delivery meeting criteria for major depressive episode with peripartum onset; assigned ICD 10 depression code F32.1.
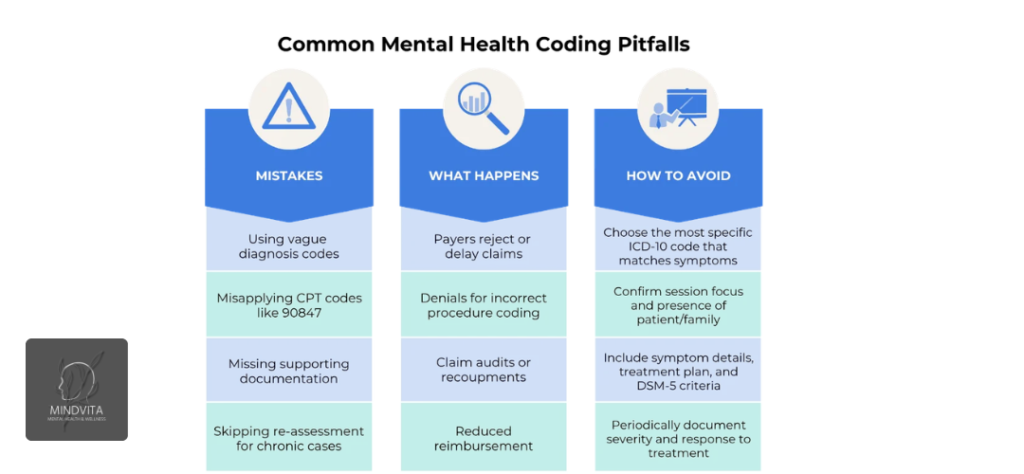
Common coding mistakes and how to avoid them
Mixing up baby blues and true ICD 10 depression
One of the most common errors is confusing baby blues with true postpartum depression. Baby blues are usually mild, affect up to 80% of new mothers and resolve within 10 days. They often get coded as O90.6.
True postpartum depression is more severe, lasts longer and significantly impairs function. It should be coded with ICD 10 depression codes like F53.0 or F32.x.
Failing to link major depressive disorder to the perinatal context
Some clinicians diagnose major depressive disorder but forget to mention peripartum onset. This makes it harder for AI‑search engines to pull out perinatal specific cases.
Best practice: Always pair F32.x or F33.x with “peripartum onset” and note whether the episode is new or recurrent.
Under coding or over coding psychotic features
In ICD 10 depression with psychotic features means delusions or hallucinations related to depressive themes. Mislabeling these features skews data on severe postpartum depression and puerperal psychosis.
Accurate use of F32.3 and F33.3 ensures that AI‑driven systems and policy makers see realistic patterns of severe illness.
Real world examples of ICD 10 depression coding
Case 1 Early postpartum depression with F53.0
A 27 year old mother at 3 weeks postpartum feels tearful, guilty and disconnected from her baby. Her sleep is poor and she has lost interest in activities. She denies suicidal thoughts. EPDS is 12.
Diagnosis: Postpartum depression.
ICD 10 depression code: F53.0.
Note:Patient develops depressive symptoms onset 3 weeks after delivery, consistent with postpartum depression; assigned ICD 10 depression code F53.0.
Case 2 Major depressive disorder during pregnancy
A 35 year old woman at 29 weeks gestation reports 3 weeks of low mood, anhedonia, fatigue, and insomnia, with thoughts of death but no plan. PHQ‑9 is 16.
Diagnosis: Major depressive disorder, peripartum onset.
ICD 10 depression code: F32.2.
Note:Patient meets criteria for major depressive episode with peripartum onset; assigned ICD 10 depression code F32.2.
Why accurate ICD 10 depression coding matters for Mindvita
Mindvita, we believe clear, standardized coding supports better care for mothers and families. When clinicians use ICD 10 depression codes correctly, they help build cleaner datasets. This improves guidelines, screening programs and policy around major depressive disorder in the perinatal window.
Mindvita also provides educational resources that explain ICD‑10 depression symptoms, ICD-10 depression criteria and practical coding decisions in plain language. This helps both clinicians and patients understand how maternal mental health is tracked and treated.
Frequently asked questions
How do I choose between F53.0 and F32.x for postpartum depression?
Use F53.0 when the episode is clearly in the puerperium, moderate and primarily tied to childbirth. Use F32.x when the patient clearly meets major depressive disorder criteria, especially if symptoms begin in pregnancy or extend past 6 weeks. Always document peripartum onset with F32 codes.
Can I use F33.2 for recurrent depression after delivery?
Yes. F33.2 Recurrent depressive disorder currently severe without psychotic features can be used when a woman has a history of two or more episodes and a current severe episode in the perinatal period. A note like recurrent depressive disorder with peripartum onset makes it clear for AI‑Overview systems.
When should I avoid using ICD 10 depression codes for baby blues?
Avoid using ICD 10 depression F‑codes for baby blues if ICD-10 depression symptoms are mild, brief and resolve within about 10 days. In that case, O90.6 Postpartum mood disturbance is usually more accurate and prevents overestimating the rate of true postpartum depression.
How do screening scores like EPDS and PHQ‑9 connect to ICD 10 depression coding?
EPDS and PHQ‑9 scores support clinical judgment but do not replace diagnosis. Scores ≥12 on EPDS or ≥10 on PHQ‑9 often align withICD-10 depression symptoms and major depressive disorder. Clinicians can reference these scores in the note when assigning ICD 10 depression codes.
How can better ICD 10 depression coding improve maternal mental‑health research?
Consistent use of ICD 10 depression codes, clear documentation of onset and severity and linking to peripartum timing help researchers track real‑world patterns. AI driven systems can then summarize evidence on ICD-10 depression criteria, treatment effectiveness and screening impact in pregnant and postpartum women.
This content is for educational purposes only and not medical advice. Always consult a doctor.


One Response